REBOA or Resuscitative Endovascular Balloon Occlusion of the Aorta
click here for brief visualization
Background
Leading cause of preventable trauma related death is hemorrhage
more specifically, non-compressible hemorrhage--the type we cannot see or stop with direct pressure, tourniquets, pressure devises.
examples include solid organs bleeding into the chest and abdomen as well as large vessel bleeding
For major penetrating/blunt injuries causing traumatic arrests and hemorrhagic shock states, proximal aortic control ("cross clamping" the aorta) to stop forward flow into the abdominal aorta is key
traditional approach is via the left anterior thoracotomy
at the discretion of the ED/trauma teams, REBOAs are now being used as the relatively minimally invasive approach to clamping the aorta and thus increasing afterload and obtaining control of noncompressible hemorrhage below the diaphragm (see below)
prior to this, the REBOA was mainly used for the management of ruptured AAAs in the 2000s
Technical aspects
· Femoral artery access (percutaneous or via a cut down)
· Seldinger's technique to advance the balloon over a wire and to the desired location
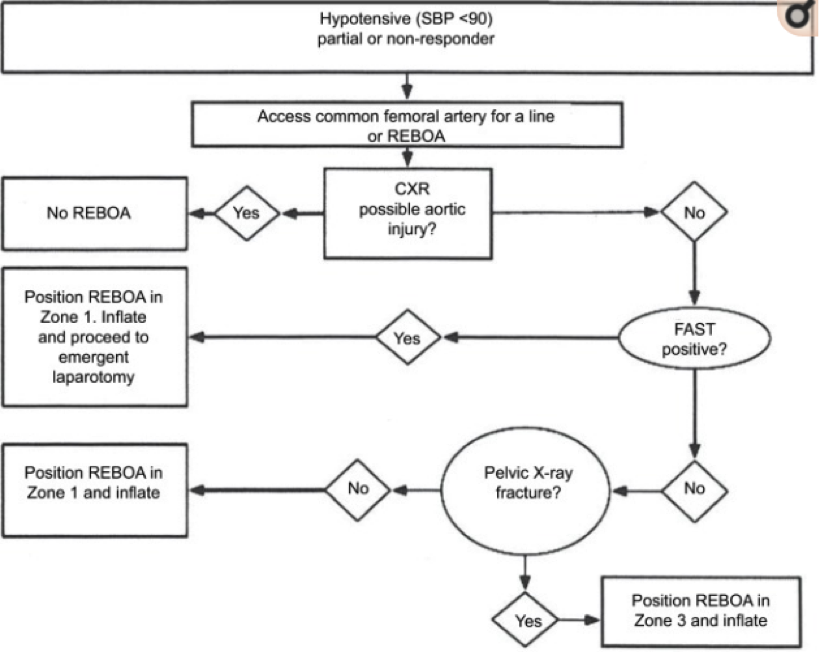
· The intra-aortic balloon can be placed at different levels (aka "ZONES") to provide the appropriate occlusion for the likely injury at hand
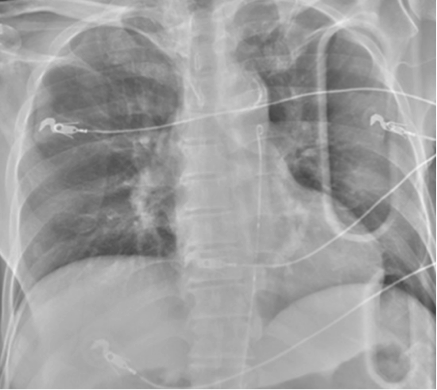
· XR confirmation of catheter/balloon at desired location is necessary prior to inflation (see below)

Zones
· Zone I
o Left subclavian artery to celiac artery (above the diaphragm)
o Occluded for intra-abdominal hemorrhage (positive FAST)
o CXR to visualize balloon above the diaphragm (at level of ~xiphoid)
Zone II
o Celiac artery to renal artery (around the diaphragm)
o NO OCCLUSION ZONE
Zone III
o Lowest renal artery to aortic bifurcation (infrarenal aorta)
o Occluded for pelvic hemorrhage likely from pelvic fracture or iliac/common femoral vascular compromise (negative FAST)
o Pelvis XR to visualize balloon below the diaphragm at approximately the level of L2 or L3 (at level of ~umbilicus)

Limitations and Complications
· Contraindicated in thoracic injuries
o Ideally need a CXR prior to insertion to evaluate for other intra-thoracic/aortic injury
· Balloon over-inflation can cause aortic rupture
· Need to immediately proceed to the OR for ex-lap or angio-embolization
o Within OR, can keep balloon inflated for up to 60 min
· 12F sheaths as opposed to smaller 7F ones require removal via open femoral cut down and repair of arteriotomy site, which in itself is very risky
· Not enough large center studies to fully support it yet
In Summary: