50 y/o male with PMHx of HTN presents to the ED s/p fall down stairs today. Patient states that he was walking to work then slipped and fell down a whole flight of stairs, striking the L side of his chest with left lateral chest pain.
Patient had left posterior and anterior rib fractures of ribs 6-10 with a small pneumothorax and some hemothorax, so the decision was made to do an Erector Spinae Plane Block for pain control.
All the clips were recorded with probe marker towards the patient's head and on the left mid-back of the patient's body.
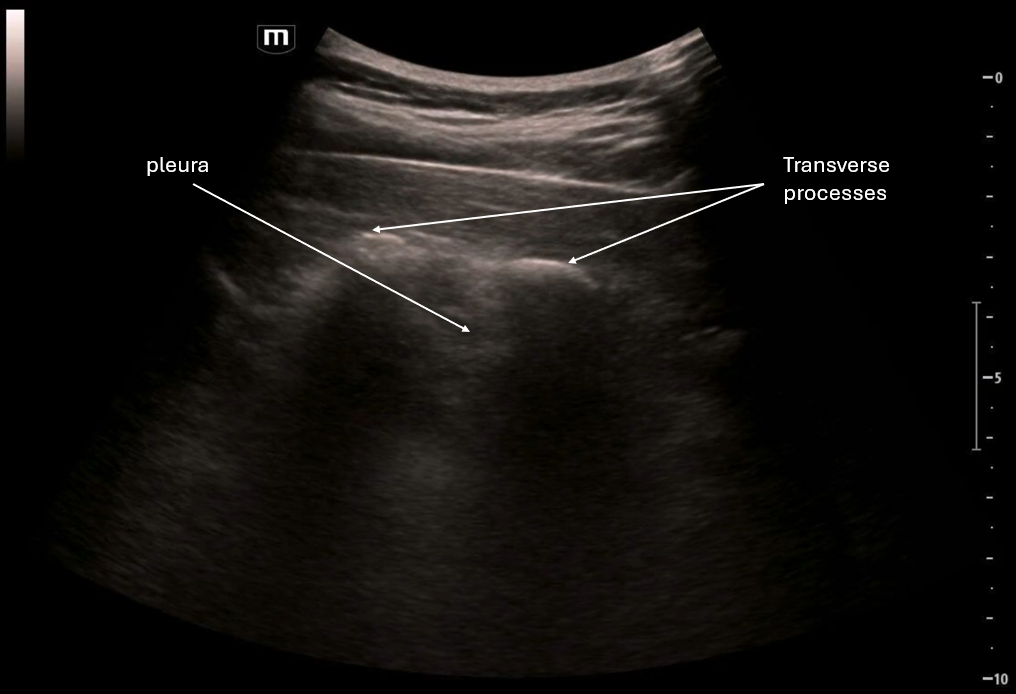
In the first clip we are looking at the landmarks of the ribs and pleura, then tracking more medially and we see the ribs become the transverse processes
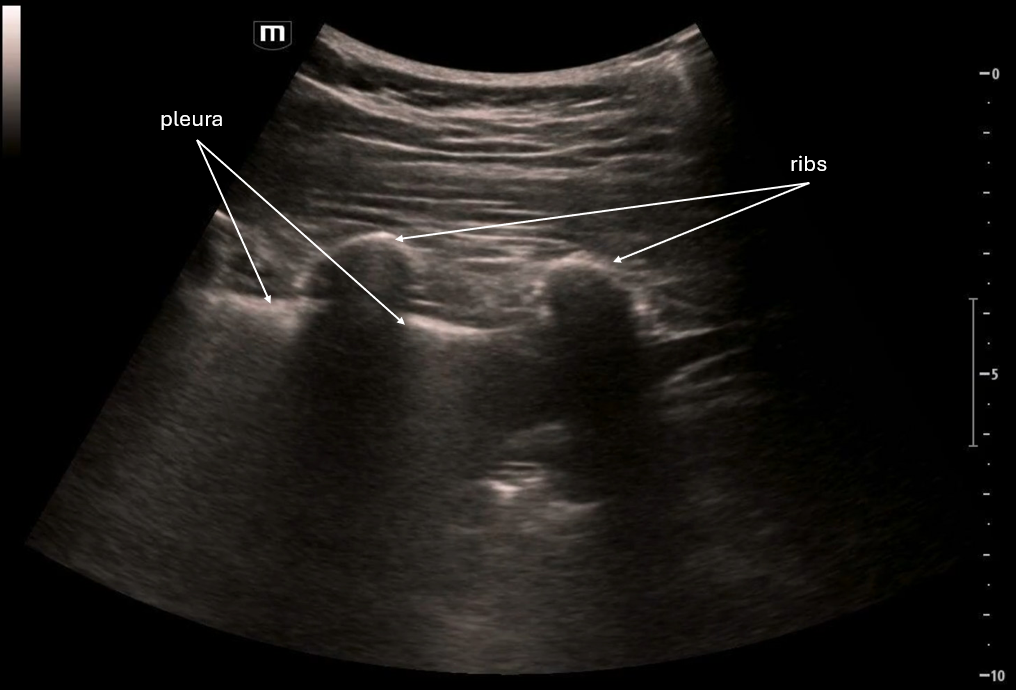
Here we are seeing the "flat" areas of the transverse processes and the hazy pleura beneath. This is where we would aim for the needle to go.
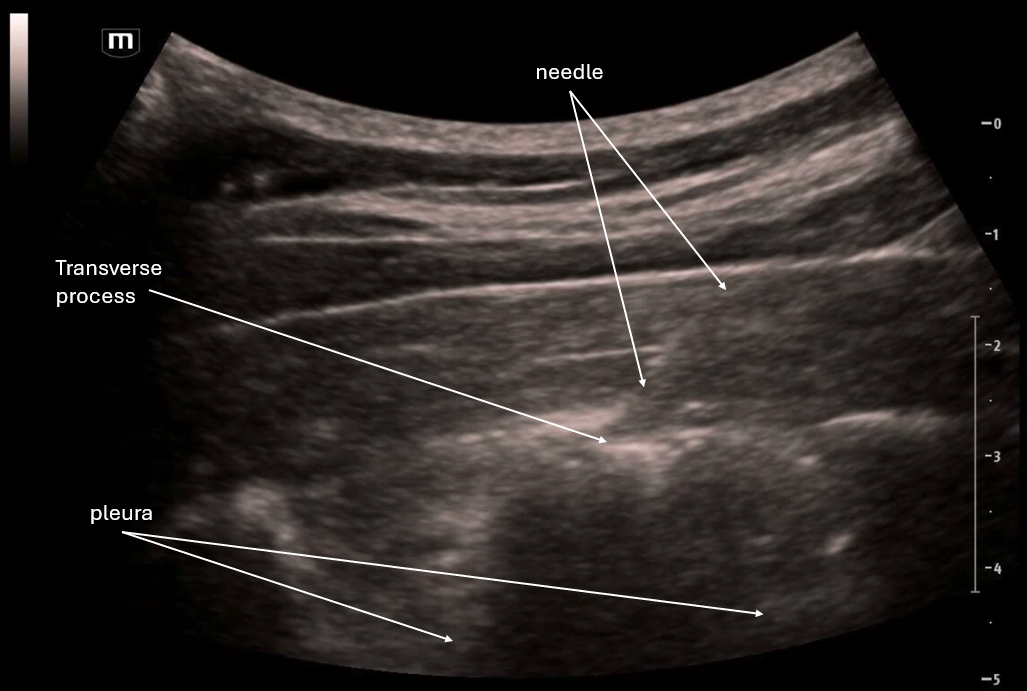
In the second and third clip we see the needle trajectory and we see the needle tip at the transverse process and injecting ropivacaine right at the transverse process and lifting the erector spinae muscle off the TP slightly.
The patient reported improvement in pain and was admitted for monitoring due to his injuries.
POCUS Pearls for Erector Spinae Nerve Blocks
Use linear or curvilinear probe positioned parasagittal 2–3 cm lateral to midline
Transverse process (TP) is the goal landmark and it is a flat hyperechoic line + shadow (NOT rib)
Muscle layers include Trapezius to Rhomboid (upper T-spine) to Erector spinae right above the TP
Targeting the plane deep to erector spinae / superficial to TP
Needle visualization in-plane until TP contact
Use 1–3 mL saline to hydrodissect and confirm plane
Visualize the fluid spread when the erector spinae “lifts off” TP
Inject 20–30 mL (adult) and continue looking for spread