This week's VOTW was brought to you by Dr. Emily Cen and Dr. Akshara Ramakrishnan!
42 y/o male with PMHx of gastric perforation (s/p repair 10+ years ago) presents to the ED sent in by PMD for abdominal pain in setting of fall of 1.5 meters at construction site 4 days ago with +FAST at PMD's office. Patient states that he went to his doctor today because of right upper quadrant abdominal pain and 1 episode of vomiting yesterday. Denies lightheadedness, dizziness, chest pain, shortness of breath.
The team did a FAST and here are some labeled images from their respective clips:
Clip 1 is a LUQ that shows free fluid below the diaphragm on top of the spleen.

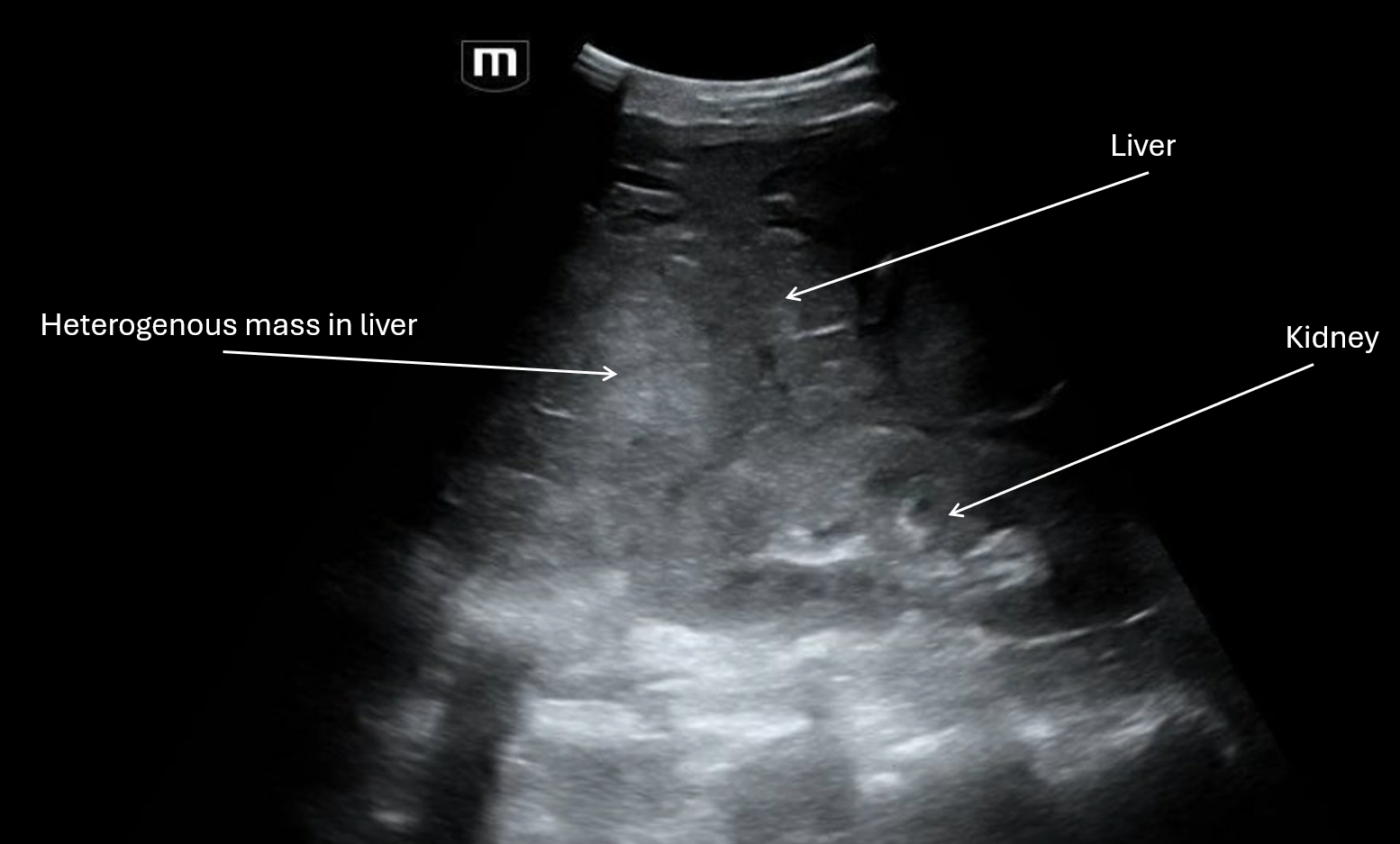
Clip 2 shows a RUQ view with the liver that appears to have a heterogenous mass.
Clip 3 shows a transverse pelvic view with free fluid in the abdomen, likely blood with a mix of fresh and coagulated blood based on the different echogenicity. Not to be confused with the bladder that is sitting right under all that free fluid and the bowel gas with dirty shadowing over to the right.

Clip 4 shows a sagittal pelvic view with bowel over to the left with dirty shadowing, again seeing the large volume of free fluid in the pelvis with the bladder off to the right of the screen.

From the imaging, patient may have liver cancer, and the trauma from the fall seemed to have caused the masses to bleed and cause large volume hemoperitoneum. IR wasn't able to identify the exact vessel that had been bleeding but empirically embolized the right hepatic artery. A total of 2 liters of bloody fluid was drained from the abdomen.
Here are some general reminders about the FAST exam:
RUQ view is most sensitive – Look at diaphragm → Morison’s → inferior kidney pole with fluid often first at liver tip
LUQ is more posterior + superior than RUQ – Look at splenorenal, subdiaphragmatic, inferior pole
Pelvis views with both sagittal + transverse – Look posterior to bladder (rectovesical)
Cardiac view can be switched to parasternal long if subxiphoid is poor – Look at pericardial vs pleural: pleural fluid lies behind descending aorta
Free fluid is anechoic with sharp angles between structures but can appear complex if clotted
FAST finds fluid, not source
Possible false negatives with early shock, retroperitoneal bleed, body habitus
References:
Kirkpatrick AW et al. Focused Assessment with Sonography for Trauma (FAST) Consensus. J Trauma. 2020.
Stengel D et al. Accuracy of FAST Meta-analysis. BMJ. 2001.
American College of Surgeons (ACS) ATLS 10th Edition.
Wish you all happy scanning!