58 y/o male with PMHx of HTN, CVA in 2013, seizures, and 40+ PPD smoking hx was transferred from outside hospital for aortic dissection. Patient reports worsening back, abdominal pain, nausea x2 days with associated bilateral lower extremity pain, weakness, and inability to walk.
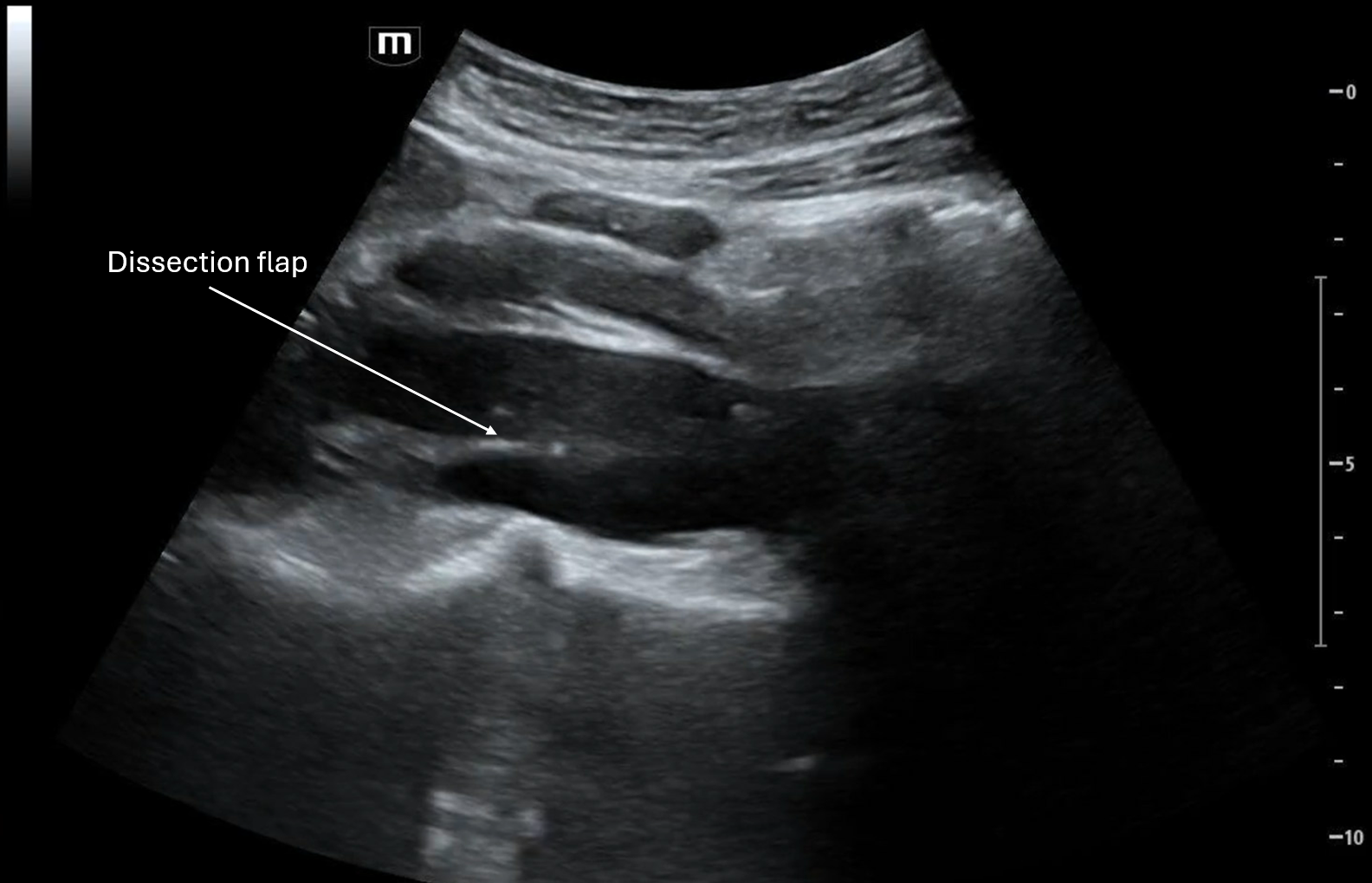
Clip 1 shows a transverse view of the proximal aortal with a dissection flap between what appears to be the true lumen and the false lumen.

As the clip goes on we see the branch points of the celiac trunk and the SMA, it appears that the dissection involves the celiac artery.


In Clip 2, the longitudinal view of the aorta includes the celiac trunk and the SMA, again it appears that there is a flap in the celiac trunk but not in the SMA.

Clip 3 is another longitudinal view of the aorta with the dissection flap.
CTA Chest/Abdomen/Pelvis revealed a type B dissection from the aortic arch to bilateral external iliacs, with a dissection flap extending into the celiac artery with SMA and R renal artery originating from the true lumen.
POCUS Pearls for Aortic Dissection
Scan the aorta in chest/back/abd pain with shock or syncope
Abdominal aorta should be < 3 cm, Aortic root should be < 4 cm
Look for dilation, flap, double lumen, and pericardial effusion
Obtain both transverse and longitudinal abdominal views of the aorta; parasternal long axis can visualize the beginning of the aortic root with the suprasternal notch view to visualize the aortic arch
Can utilize color doppler to distinguish true lumen (faster flow) from false lumen (slow/swirling)
Red flags: aortic root dilation + pericardial effusion → Type A dissection until proven otherwise
Negative POCUS ≠ rule out aortic dissection, CTA if clinical suspicion is high
If you see anything abnormal → escalate immediately
References:
Nazerian P et al. POCUS protocol for acute aortic syndromes. Acad Emerg Med. 2019.
Moore CL et al. US in aortic emergencies. Acad Emerg Med. 2007.
Evangelista A et al. Key imaging findings in acute aortic dissection. Circulation. 2003.
Kimura BJ. Focused echo for aortic root dilation. JASE. 2012.
Nienaber CA & Clough RE. Acute aortic syndromes overview. Lancet. 2020.