40 y/o male with no PMHx presents for sudden visual changes in the right eye starting yesterday morning with blurry vision in the inferior visual field of the right eye. States that he was seeing "white bubbles,” and a “wave” that is black with some red discoloration. Reports that the vision changes worsened acutely with the "dark area" appearing to expand upward. Denies eye pain, trauma, or prior similar episodes. States that he wears glasses at baseline with no other ocular diseases.
In Clip 1 there is a thick bright hyperechoic line that extends from the optic disc, very much tethered to the back of the eye ball, that is the retina that has detached from the back of the eye.
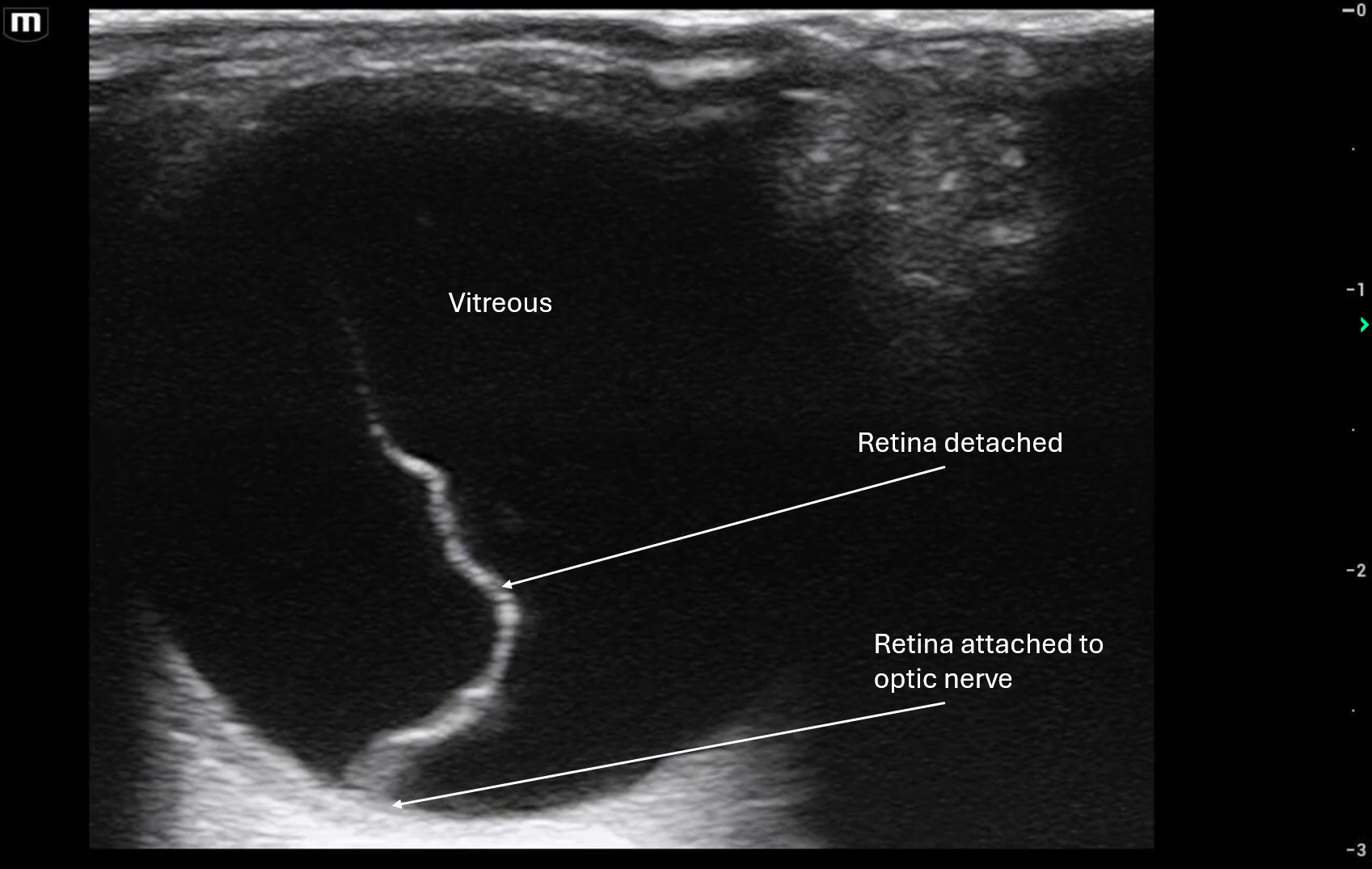
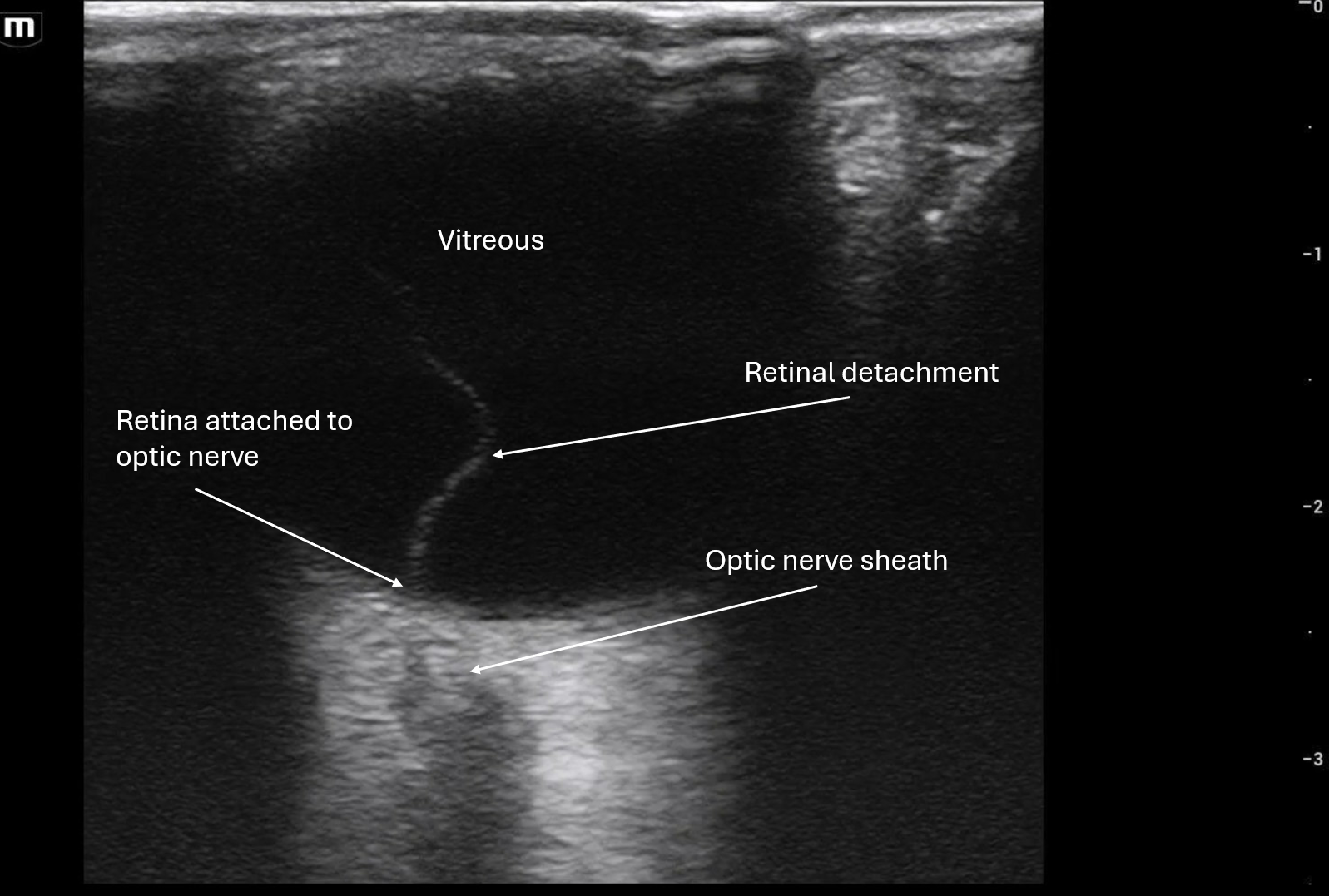
In Clip 2 it shows that the retina does seem attached to the optic disc because you can see the optic nerve sheath in this image.
In both clips you can see that when the patient moves his eye, the retina is mobile but attached to the optic disc/back of the eye. This is concerning for retinal detachment until proven otherwise!
Patient was transferred to outside hospital to Ophthalmology for retinal detachment.
POCUS Pearls for Retinal Detachment Ocular Ultrasound:
Hyperechoic, thick linear membrane within the vitreous
Tethered to the optic disc (key distinguishing feature)
V-shaped, Y-shaped, or funnel-shaped configuration in larger detachments
Limited mobility with eye movement (moves less than vitreous debris)
Often described as a “sail” or “curtain” floating in the posterior chamber